Something
for which I was never prepared when I joined NJH in June 2010 was the amount of
critical care work which I would end up doing.
Having
a background in Community Medicine (Public Health), it was a challenge to get
into using ventilators, managing pulmonary edema, rupture uteruses, cerebral
malaria. More of a challenge since my last year in the Christian Medical
College, Vellore was spent among the Jawadhi tribal community trying to
convince them to come for antenatal check-ups, getting them to run small scale
income generation programmes, conducting mobile health clinics etc.
From
an healthcare institution point of view, NJH was quite peculiar.
Situated
in the middle of a heavily forested area along a National Highway linking
Ranchi with Gwalior, one would have expected hardly much of a crowd. Yeah, we
do not get much of a crowd. The routine cases of malaria, enteric fever and
normal deliveries are dealt by the motley crowd of quacks and dais in the
villages.
So,
if you come to our outpatient, you may think that there is not much work. But
our repertoire of cases will put a Medical College to shame. You want to know,
what we have in our 6 bedded Intensive Care Unit now. Here’s the list –
1. A young man who’s survived
a krait bite. He was in the ventilator for about a fortnight. Then he went into
pulmonary edema. He’s slowly on his way to recovery.
2.
A
young lady who went into pulmonary edema following eclampsia. She lost her
baby. We had very little hope of salvaging her.
3.
A
middle aged woman with organophosphorus poisoning. Again, we were not very sure
of getting her alive. She had drunk too much of poison. She’s also slowly
recovering.
4.
A
little girl with partially treated meningitis. Still not very sure of what the
outcome will be.
5.
A
young man who’s just come in with a clinical diagnosis of cerebral malaria. For
him to be admitted, we had to shift out a young lady who had a molar pregnancy.
She had a hemoglobin of 2 gms%. By God’s grace, we could do an evacuation and
she’s doing ok.
6. An elderly lady with a very
bad pneumonia. She has already been managed at Ranchi.
Then
there are 3 more patients with severe malaria who are waiting in the General
Ward. I would have wanted them also to be under close observation. In addition,
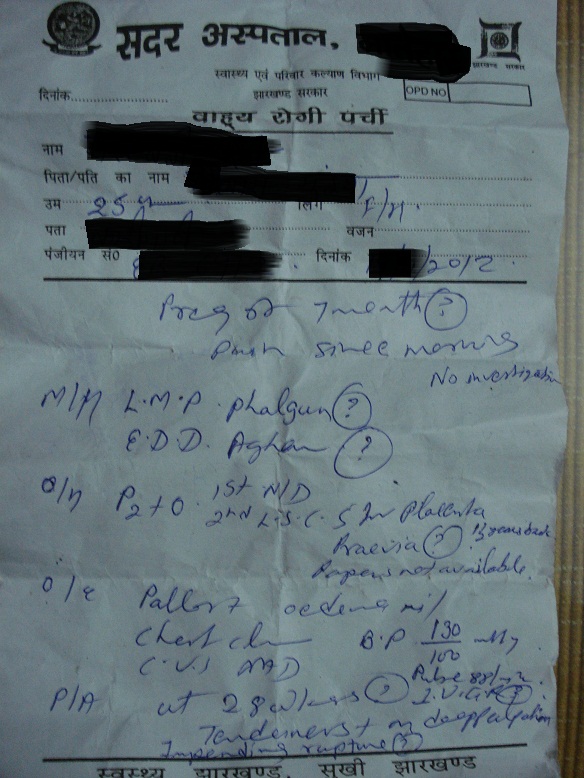
there is a young lady with bad obstetric history (G6P5L1D4) having severe
pre-eclampsia at 28 weeks who’s refused to go elsewhere.
I
can only pray that there is no patient with rupture uterus or eclampsia coming
in during the next 24 hours.
Well,
what do I want to convey?
Critical
care is something that we in mission hospitals need to look at very seriously.
Traditionally known to be bastions of surgical care, there has been a major
shift.
The
major reason being that very few hospitals are interested in critical care and
when there are facilities for critical care, it is too expensive for the common
man.
So,
along with palliative care, geriatric care, care of HIV AIDS etc . . . something
very unusual is being expected from us in the form of critical care.
However,
the ultimate question is about getting committed young men and women to serve
alongside us.