Few days back, one of my senior colleagues shared an article on how deaths from heart attacks have dramatically come down in the United States. However, as I read it I know very well that only a minuscule of patients in our country who suffer a heart attack would ever undergo emergency angioplasty.
Angioplasty - that's the name given to the way they save the heart by opening the blocked artery by pushing in a catheter, inflating a tiny balloon and inserting a stent which will keep the artery wall patent. And this has to be done fast . . . very fast.
Take the example of 2 patients whom I saw in emergency over the last couple of days at KCH. We worked fast to ensure that both the patients are referred to a higher centre. When we referred, the minimum we expected was that both the patients would be given Streptokinase to dissolve the block in their coronary artery.
The first patient, a 38 year old mother of three with well documented anterior wall myocardial ischemia, was prescribed Aspirin, Atorvostatin and Clopidogrel and sent back home.
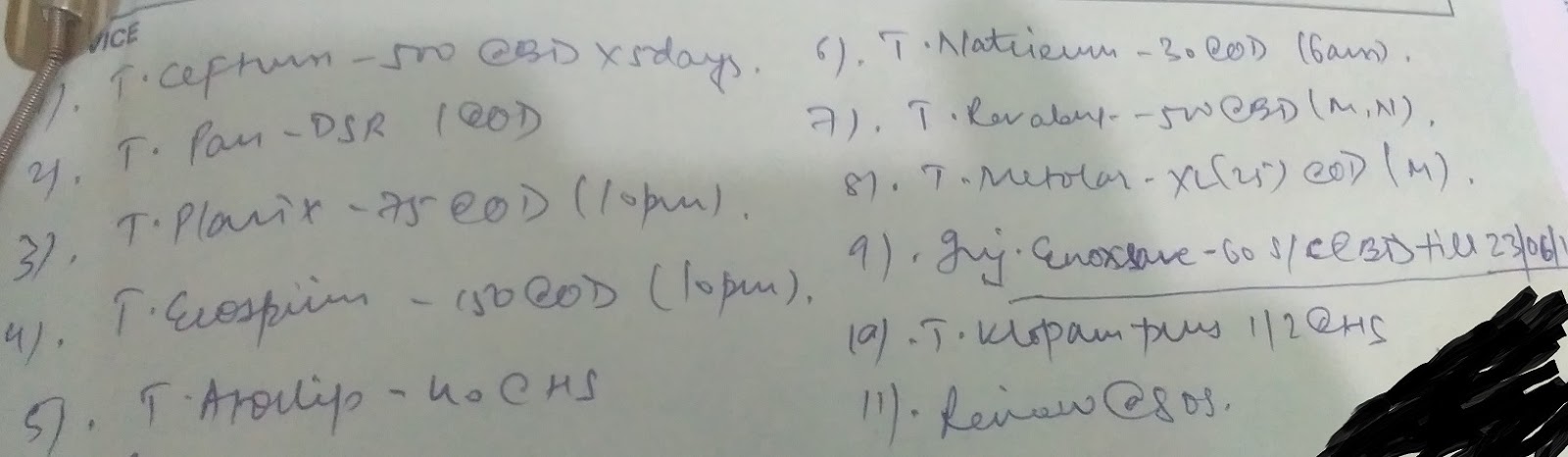
The second patient was a 60 year old gentleman with typical symptoms of Myocardial Ischemia. He did not have typical features on ECG, but since the symptoms were typical, we referred him. Couple of days, the relatives came back saying that he had a heart attack with elevated enzymes.
The guy was luckier as from the prescription, it seems that he got low dose heparin.
There are 2 aspects.
The first is the cost involved in treatment. The latter patient incurred a cost of 60,000 INR for treatment at the cardiac specialty centre he went to for a 3 day stay. No small amount for a middle class family, leave alone for the majority of my fellow citizens.
The second aspect being the number of intervention cardiologists available in the country. I wonder if the total number of intervention cardiologists in the whole country is even a 4 digit number.
The third aspect is about where you'll be treated. The first patient was seen by cardiologists in a public healthcare set up. The second patient in a private tertiary cardiology care centre.
The third aspect is about where you'll be treated. The first patient was seen by cardiologists in a public healthcare set up. The second patient in a private tertiary cardiology care centre.
When we look at it - Yes . . . there's a lot of people dying out there or more than that getting debilitating heart damage due to ischemic heart disease, all because of high costs and non-availability of specialists.
Well, the future looks bleak in a country which is still grappling with maternal deaths, children dying of diarrhoea and respiratory tract infections, tuberculosis and malaria.
As for the time being the best option for us remains -
2. Good exercise
3. Control of risk factors such as diabetes and hypertension.
From the policy, we would need to see -
1. If thrombolysis treatment can be authorised in primary care.
2. Short courses for medicine consultants in the public health secondary care institutions to do angioplasties.
Till those happen, the 3 cardinal rules to have a healthy heart remains the best option in the country . . .
Till those happen, the 3 cardinal rules to have a healthy heart remains the best option in the country . . .
Do you need Finance? Are you looking for Finance? Are you looking for finance to enlarge your business? We help individuals and companies to obtain finance for business expanding and to setup a new business ranging any amount. Get finance at affordable interest rate of 3%, Do you need this finance for business and to clear your bills? Then send us an email now for more information contact us now via financialserviceoffer876@gmail.com whats-App +918929509036 Dr James Eric Housing Finance Pvt Ltd Thank
ReplyDelete